幅広い人間理解を得るために必要なこと
富士市富士宮市にて在宅医療に携わっている薬剤師の栗原です。
今日は「薬歴」について書きたいと思います。
目次
1) The Basic Contents of a Medication Record
3) Comparing Paper Medication Records and Electronic Records
4) Learning How to Document Medication Records
5) Documenting Medication Records as Part of Patient-Centered Work
6) Revisions to Medical Fees Also Reflect Patient-Centered Work
8) Medication Records Based on “One Problem”
9) Guidance Amid Complex Backgrounds
10) Flow of SOAP Documentation
11) Don’t Discard the Long Tail in Medication Records
13) Medication Records Are Tools for Patient Benefit
14) Timing of Medication Guidance
1)薬歴の基本的な中身
薬歴というのは、薬剤師が患者様に処方箋に基づいてお薬をお渡ししたのちに記す記録のことです。この薬歴を記録しておくことが、患者様からお薬代を頂戴する上での必須要件ともなっております。内容は、
・患者様のお薬の服用状況や服用後の様子
・既往歴や現病歴
・服薬指導並びに指導計画
・副作用歴
・併用薬(健康食やOTC医薬品を含む)
・住所、電話番号などの連絡先
・保険情報
などとなっています。
2)薬剤師の2W1H
薬剤師は処方箋に基づいたお薬を投薬するたびにこの薬歴を記載します。そのため、1人の患者様が、
1)どのような症状で(Why)
2)どのようなお薬を(What)
3)どのようにして投薬したのか(How)
ということについて、過去に遡って辿ることが出来ます。
薬歴そのものは「SOAP」式という記載方法で記録されますが、このようにして記載された薬歴を読み解くためにこの3つの視点はとても大切です。何故ならこの視点を持つことで、薬歴の形式に囚われずにその中身を検証することが可能になるからです。【薬剤師の2W1H】としてぜひ意識づけしていただきたい。
注)一般にはPOSシステムという試行方法が医療現場で用いられています。問題志向型システムと呼ばれるもので、患者様の抱えている課題(問題)に基づいて医療的介入を描き出す。
「情報収集」
→「問題の明確化」
→「解決のための計画立案」
→「計画の実施」
上記で提案した2W1Hは、この問題解決のための手続きを簡素化したものと言えます。簡素なスタイルだからこそ一度習得すればさまざまな面で応用できます。
3)紙の薬歴と電子薬歴の比較
現在はほとんどの保険薬局で電子薬歴が用いられています。それまでは紙の薬歴という形で保管されてきました。
紙の薬歴には紙の良さがありました。何より一覧性が高く、ページをめくれば視覚性の良い状態で患者情報を辿ることが出来ます。細かくメモ、記載された情報から、色々と患者様について黙想することができる。
それに対して電子薬歴は、
- 一覧性を高めるには細かな設定、管理が必要
- 使い慣れるのにそれなりの手間と時間がかかる
- 入力した情報の修正に一手間かかる
- 患者情報を辿っていくのに、少し手間がかかる
などのデメリットがあるものの、
- ・処方箋に記載されたお薬の添付文書の情報をすぐに開くことができる
- データベース化されたお薬の相互作用、副作用情報がAIの助けを借りて調べられる
- 保存情報が劣化しない
- 薬歴の記載漏れを防ぎやすい
というメリットがあります。今後、電子薬歴の活用は必須となっていくでしょう。
4)薬歴の記載方法を学び取る
調剤薬局の薬剤師は日がな一日、この「薬歴」に向かい合うことになります。平均的に薬剤師は1日に30枚程度の処方箋を取り扱うため、30回、薬歴を記載することになります。
30枚の薬歴を、意味のある整合性の取れた薬歴に仕上げることは、そう簡単な話ではありません。薬剤師の知識、知見の程度によって、当然、その内容の充実度は異なってきます。薬剤師として、患者様とどれだけ適切な関係を保ってあるかが如実に出る。1枚の処方箋に基づいて相応しい投薬をしたかどうかが、その薬歴を見ればかなり見えてくるのです。
薬歴の書き方については、薬学部では基本的な事柄は大学で学びますが、実践的には現場に出てから学びます。薬歴の書き方については多くの書籍があります。それらを参考にして、気に入った解説があればそれを徹底的に実践してみることでこそ身につくというものです。多くの新米薬剤師は、現場に出て先輩からのフィードバックを繰り返し受けて、ようやくこの書き方を身につけていきます。
ただし薬歴の書き方の習得レベルについては、職場の教育環境によってかなり程度の違いが生じているようです。
ですから今回はこの薬歴について、
・どのように書けば最も整合性のある薬歴となるか?
・薬歴を介してどのように患者様の利益に結びつけていくことが出来るのか?
という実践的な側面に着目しながら解説していきたいと思います。
5)対人業務に基づく薬歴の記載方法
近年、薬剤師に、より根拠のある「対人業務」としての医療的介入の務めが求められるようになってきました。患者様の検査データや患者の体調という、医療的で科学的根拠に基づく服薬指導管理が要請されている。
患者様が「どのような課題を抱えているか?」、それに対して薬剤師が「どのようにアプローチ(服薬指導)したのか?」を明確に記録することが求められるようになったわけです。薬歴という点で言えば、1つの薬歴をそれ自体で完結したものとせずに、「どのように次回の服薬指導に繋げていくか?」という患者様へのフォローアップが要請されるようになってきました。
6)診療報酬の改正にも対人業務の項目がある
薬局が対価として得る代金の基準である診療報酬の設定においてもそれは明確です。
「もの」であるお薬そのものをピッキングして取り揃える対価が「調剤技術料」ですが、改訂によってこの割合が低下し、患者様一人一人の併用薬、薬疹歴、アレルギー歴や体質、生活習慣と服薬との関係をチェックする「調剤管理料」が設定されました。
「調剤技術料」が物に対しての報酬であるとすれば、その物である薬物を患者様が実際に服薬する「薬と患者の関係」について考察する対価が「調剤管理料」です。
加えて、薬剤師の働きは患者様がお薬を口に運ぶまでが管理の対象なのではなく、服用後の状態・様子もフォローすることが求められています。たとえば糖尿病治療薬であるインスリン製剤の導入や用法用量・種類の変更があった場合には、使用後の状態を電話等の連絡手段で確認することが求められるようになりました。それが「服薬管理指導料」です。言ってみればこれは完全な「対人」の働きが薬剤師に明確に求められるようになったということであり、平成4年度の医療法の改正によって薬剤師もまた明確に医療者として位置付けられたことに対応しているものと言えます。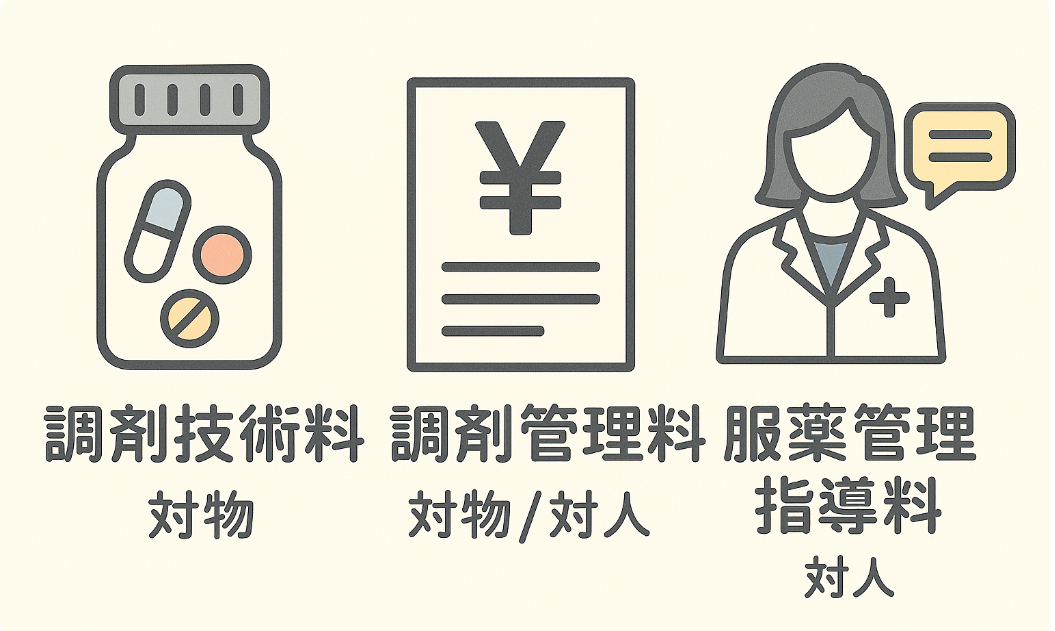
これにより、薬歴は単なる「投薬記録」ではなく、これによって患者様に薬学的な貢献をするための不可欠なツールとみなされるようになったと言えます。
7)SOAPを理解する
薬歴にはある程度、「形式」が必要とされます。記録者が全く自分の形式で記録すると、他の薬剤師がその患者様に投薬をする際に不都合が生じることになるからです。
一般的に薬歴は「SOAP(ソープ)」という形で整えられます。
SOAP記録フォーマット
S (Subjective) — 主観的情報
・患者の訴え、自覚症状
・体調変化に関する本人の表現(例:「眠気が強い」「食欲がない」「動悸がする」など)
・病院を受診するに至った経緯や生活背景
⸻
O (Objective) — 客観的情報
・血液検査データ、バイタルサイン
・処方内容の変更点や特徴(新規薬、減量、中止など)
・薬剤師から観察できた患者の状態(例:顔色、歩行、言動など)
⸻
A (Assessment) — 評価・考察
・薬剤師による薬学的評価
・薬物療法に関する考察(相互作用、副作用リスク、コンプライアンスの課題など)
・患者分析、服薬継続における懸念点や記録すべき事項
⸻
P (Plan) — 計画
・実施した服薬指導の内容
・今後の指導や確認事項(例:次回までに副作用の有無を確認、服薬アドヒアランスのチェックなど)
・医師への情報提供が必要な場合の対応方針
以上のように了解することができるでしょう。
8)One problemに基づく薬歴
薬歴は「One problem」に基づいて記載されなければならないと言われます。服薬指導をするにあたっての主題ならびに主眼がどこにあるのかを明確にすることが求められている。
かと言って、「これが主眼だ」と言葉に明確にする必要はありません。何故なら服薬指導における主眼は、あくまでも複数の因果関係の中にあって、あえてどの点に焦点を絞って服薬指導したか?を意味するものだからです。SOAPという形をとった薬歴「全体」で、それが浮かび上がれば良い。
9)複雑な背景の中での服薬指導
薬剤師としての力量が試されるのは「A」です。薬学的に理屈の通る分析は、それぞれの薬剤師の賜物が明確に現れる箇所です。
服薬指導は複雑な背景のもとになされるものです。患者の症状の変化、自覚症状、本人は自覚できない症例(慢性病の多くはそのようなものです)・・。処方箋1つとっても、薬剤は多岐に渡る。降圧剤もあれば脂質異常症のお薬がある・・。そういった中で、あえて「今回」、どのプロブレムに着目して服薬指導したのかを可能な限り明確に浮かび上がらせる必要がある。
1人の患者様は、通院という形で繰り返し来局し、薬を受け取ります。その際、毎回、同じ服薬指導をすることは、あえて避ける必要があるとも言えます。あえて別な視点から患者様にアプローチすることで、それまで見えなかったことが見えてくることもある。当初の情報(患者様の初回情報)には、併用薬や嗜好品、生活習慣やアレルギー歴の記録はなかったけど、角度を変えた質問でそれが初めて分かるような事例もあります。
それまで患者様が薬剤師や薬局に心を閉ざして情報を提供していなかったということもある。患者様が薬剤師という職能の持っている役割を理解していなかったということもある。ですからあえていつもとは違ったアプローチをとって、関係性(信頼関係)を強め、日常会話からコミュニケーションを行うことが有効です。それは薬歴を充実した、生き生きしたものに変えることがある。
10)SOAP記載の流れ
薬歴の形式のSOAPは、主訴(S)に対して、それと関連のある事実(O)を提示し、薬学的考察(A)を行い、どのような指導(P)を行うかのについて、一連の流れを待つべきです。それが一貫性のある薬歴の原理的側面である。
この視点に立ってchatGPTに具体的な薬歴を書いてもらいました。
SOAP記録の流れ(例)
S(Subjective:主訴)
「最近、夜眠れない。薬を飲んでも寝つきが悪い。」
⸻
O(Objective:客観的事実)
・現在処方:睡眠導入剤(ゾルピデム 5mg 就寝前)
・処方開始は2週間前
・来局時の様子:やや疲れた表情、日中の眠気なし
⸻
A(Assessment:薬学的考察)
・効果不十分の可能性。耐性や依存のリスクを考慮しつつ、まずは服薬状況・服薬タイミングを確認すべき。
・飲酒やカフェイン摂取など生活習慣の影響も考えられる。
・増量や薬剤変更の検討は医師判断が必要。
⸻
P(Plan:指導・計画)
・就寝直前に服用しているか確認。今後も就寝直前の内服を徹底してもらうよう指導。
・寝る前のカフェイン摂取やスマホ使用を控えるよう生活指導。
・次回来局時、効果の有無を再度確認。改善なければ医師に情報提供を検討。
⸻
このように、患者の主観的な訴え(S) に対して、関連する客観的事実(O) を提示し、それをもとに 薬学的な考察(A) を行い、最終的に 具体的な指導・計画(P) を記録することで、ストーリー性のある薬歴になります。
薬歴としては理想的なスタイルを持っていると納得していただけると思います。
11)薬歴におけるロングテールを切り捨てない
ただし、現実はこのように一貫性のある薬歴が書けるとは限りません。患者様が受け答えに乗り気でない場合もあります。ですからこの筋道にこだわりすぎると、せっかくの患者様から聴取した情報を記録し忘れることにも繋がります。
意味のある薬歴を記録することは薬剤師の務めですが、あえてその際には「その時には意味(価値)がないと思える情報」も記録しておくことも、その後の薬歴に役に立つことがあるものです。
イギリスの経済学者のヴィルフレド・パレートは「パレートの法則」というものを提示しました。例えば売り上げの世界では、2割の商品が、全体の売り上げの8割を充当させるという法則です。
服薬指導に関して言えば、患者の訴えの中でお薬に関係する部分は会話の2割程度。それが重要度で言えば全体の8割を占めます。ですが、残りの8割(これをロングテールと言います)の部分が、後々になって意味を持つことがある。
1人の患者様に服薬指導するにあたってもっとも重要なことは、日々の血圧の変動や血糖値の変動、体の調子、自覚症状などであることは間違いありません。でも、それ以外にも、その時には意味をなさなかった食生活や生活環境の変化、職場の移動などが、患者様の症例に対して、後から大きな影響をもたらすということがある。
ですから「S」や「A」には、一見関係のない情報も記載しておくことをお勧めします。
12)SOAPの肝
・・でもそれでは一貫した意味を持つ薬歴にはならないのではないか?と思われるかもしれません。それは薬歴とは言えないのではないか?そう思われるのも仕方ありません。
ここで大切なことは、薬歴を構成する「S」「O」「A」「P」に関して、少なくとも「O」と「P」の対応関係はつけておくということです。
「起承転結」で言えば、「承」と「結」は、必ず対応しなければなりません。この対応関係の崩れた薬歴は空中分解している状態です。よく出来た四コマ漫画も、二コマ目の「承」と四コマ目の「結」が必ず対応関係にあります(この点でお手本とすべき四コマ漫画は植田まさしさんの『コボちゃん』や『かりあげクン』です)。
13)薬歴は患者様に貢献するためのツール
しかしさらに、薬歴を書く上でとても大切なことがあります。それは、薬歴とは、あくまでも薬剤師にとって患者様の服薬管理を行うためのツール(道具)に過ぎないという視点です。
つまり薬歴は、ストーリーや形が本質的に重要なのではなく、それがどの程度、患者様とのコミュニケーションや服薬指導のツールとして機能しているか?ということに着目することが大事です。
一見、守備一貫せず、尻きれトンボの薬歴があるとします。
患者様が急いでいて必要最低限のことも聴取できなかったとか、薬剤師に対して不信感を持っているのか質問に答えてもらえないといった場合です。でもその薬歴は、そのままの形で残して、次につなげる形をとれば良い。あえて中身のない、本当は指導していないような内容を記載するよりは、事実ベースに書いて、その後のフォローアップに繋げていけば良い。大事なことは薬歴そのものにあるのではなく、それを通してどの程度、患者様の薬物治療に関与する意思を持っているか?なのです。
本来なら患者様から聴取しておくべき事柄を聴取できなかったとしても、それを憶測で書いてしまうのではなく、それはそれとして、次回以降の課題として残し、次の指導に生かすべきと受け止めることが大事です。
14)服薬指導のタイミング
いつのタイミングで服薬指導を行うのか?
薬歴について考える時に、しばしば見落とされてしまうのが、実際の投薬と薬歴の有機的な関係です。これが見えていないと、実際の投薬と薬歴の内容が乖離することになる。そのような薬歴をどれだけ残しても、全く患者利益にはならない。
実際に薬歴を書く事情に照らして、この関係について考えなければなりません。
1人の患者様の薬歴を完結させるためには、最低、5分はかかるものです。電子薬歴を見ながら、新しい処方内容を吟味し、過去の患者様情報と照らし合わせ、投薬(服薬指導)にあたります。すなわちお薬の監査から既に薬歴は始まっています。
理想的には患者様が薬局に入ってきた時点で、今回来局(受診)された事情を聴取しておくことです。そうすればお薬の監査の段階において、すでに薬学的な考察はかなりのところまで進めることができます。
ですが現実には、薬剤師は投薬の段階で初めて患者様と顔を合わせて、状態や主訴を確認出来ます。ですから過去の薬歴から推察して、今回の処方から、患者様の状態、背景について推察します。そして、ある程度服薬指導の目安(当たり)をつけて患者様対応に臨む。こういう一連の思考の流れが出来なければ、出たとこ勝負になり、充実した服薬指導はできません。
15)仮説を持って患者様に望む
服薬指導の目安(当たり)とは、言ってみれば「仮説」です。
今回、この患者様はどういった事情で病院を受診し、その結果このお薬が処方されたのではないか?ここで薬剤師としての経験値が顔を出す。薬剤師は自分の経験の積み重ねの上に、目の前の患者様を対応する。結果として、日々の業務そのものが学びの機会となる。
処方箋を受け取ってお薬を調剤したら、処方箋の内容、お薬手帳、過去の薬歴と睨めっこをして、「当たり」をつけて患者様の前に出る。そこから患者様から直接、聴取を行い、その処方箋の内容で疑問点はないか?薬学的な観点から確認すべきことはないか?などを考えながら投薬することになる。
でも「当たり」が違うこともある。患者様から想定外の情報提供があることもある。その場合、「仮説」を修正しつつ、改めて新しい情報と、それに対する薬学的考察を行って、投薬することになります。
また次回以降、患者様から確認すべき事柄に関して特化すべきことがあれば、それも書き残して、次回の薬歴に反映させる必要があるのです。
16)薬剤師の哲学を持つ
このような薬歴の記載を、普通の薬剤師は1日に30回くらいしている。これは大変なことです。だから薬歴の記載方法に関しては、自分なりの哲学を持たないといけない。
ここでいう【哲学】とは、単純な記録の記載行為を意味あるものとするための理解力のことです。また服薬指導という【実践】を実りあるものとする思考の枠組みのことです。
一歩、後ろに下がって思考を巡らし、実践に移すこと。そのためにSOAPの仕組み、並びにその実践的な課題について、自分の理解力の中に落とし込まなければならない。この記事がそのために役に立てば幸いです。
I am Kurihara, a pharmacist involved in home medical care in Fuji City and Fujinomiya City.
Today, I would like to write about “Medication Records (薬歴).”
[[Table of Contents]]
1) The Basic Contents of a Medication Record
A medication record (薬歴) is a record written by the pharmacist after dispensing medicines based on a prescription to a patient. Keeping this record is a mandatory requirement in order to receive payment for the medication from the patient. The contents include:
・The patient’s medication adherence and condition after taking the medicine
・Past medical history and current medical history
・Medication guidance and instruction plan
・History of side effects
・Concomitant drugs (including health supplements and OTC drugs)
・Contact information such as address and phone number
・Insurance information
2) Pharmacist’s 2W1H
Pharmacists record a medication history each time they dispense medication based on a prescription. This allows us to trace back for each patient:
・Why — What symptoms the patient had
・What — What medicines were dispensed
・How — How the dispensing was carried out
Although medication records are kept in the “SOAP” format, this perspective (2W1H) is crucial for interpreting them. Why? Because with this perspective, we can evaluate the contents without being constrained by the SOAP format itself. Please remember this as 【Pharmacist’s 2W1H】.
3) Comparing Paper Medication Records and Electronic Records
Today, most community pharmacies use electronic medication records, but in the past, they were kept on paper.
Paper records had their advantages. Above all, they offered excellent overview: flipping through pages allowed pharmacists to follow patient information visually, and one could reflect on the patient based on handwritten notes.
On the other hand, electronic medication records have some drawbacks:
- ・To enhance overview, detailed settings and management are required
- ・It takes time and effort to get used to the system
- ・Editing entered information requires extra steps
- ・Tracing patient information can take extra effort
Nevertheless, they also bring advantages:
- ・You can immediately open package insert information for prescribed medicines
- ・Drug interactions and side effect information can be checked with the help of AI databases
- ・Stored information does not deteriorate
- ・Helps prevent omissions in documentation
Thus, despite drawbacks, the use of electronic records is indispensable going forward.
4) Learning How to Document Medication Records
Pharmacists in community pharmacies spend much of their day working on these “medication records.” On average, a pharmacist handles about 30 prescriptions per day, which means documenting about 30 medication records daily.
Writing 30 meaningful and consistent records is not easy. The depth and quality naturally vary depending on the pharmacist’s knowledge and insight. It clearly reflects how appropriately the pharmacist has engaged with the patient. By looking at a medication record, one can often see whether the pharmacist provided proper dispensing based on the prescription.
Many books explain how to write medication records. Learning comes from referring to them and practicing thoroughly. However, most novice pharmacists acquire the skill through repeated feedback from senior colleagues in practice.
That said, the quality of training varies significantly depending on the workplace environment.
In this article, I would like to focus on the practical side of:
・How to write the most coherent medication records
・How to link medication records to patient benefit
5) Documenting Medication Records as Part of Patient-Centered Work
In recent years, pharmacists are increasingly expected to provide evidence-based patient-centered interventions. This includes incorporating test data and monitoring patient conditions into scientifically grounded medication guidance and management.
It is now required to clearly document what issues the patient faced and how the pharmacist approached them through guidance. A medication record should not simply end with one encounter but should show “how the guidance connects to the next visit”.
6) Revisions to Medical Fees Also Reflect Patient-Centered Work
This is evident in the revision of medical fee structures, which determine how pharmacies are compensated.
The payment for physically preparing and dispensing medications, “dispensing technical fee”, has been reduced in proportion, while a new category, “dispensing management fee”, was established. This fee accounts for checking each patient’s concomitant drugs, allergy history, constitution, and lifestyle in relation to medication.
If the “dispensing technical fee” is a fee for the “object” itself (the medicine), the “dispensing management fee” is a fee for considering the “relationship between the patient and the medicine”.
Furthermore, pharmacists are required not only to manage until the medicine reaches the patient’s hand, but also to follow up on the patient’s status after taking it. For example, when insulin is newly prescribed or dosage/type is changed, pharmacists must follow up by phone or other means. This is the basis of “medication management guidance fees.” It demonstrates how pharmacists are now explicitly required to provide “patient-centered” work, consistent with the 1992 Medical Law revision that formally recognized pharmacists as healthcare professionals.
Thus, medication records are no longer mere “dispensing notes” but have become an indispensable tool for contributing to patient care pharmacologically.
7) Understanding SOAP
Medication records require a certain degree of “format.” If each pharmacist wrote records in their own style, it would create problems when other pharmacists later dispensed medication to the same patient.
In general, medication records are organized in the form of “SOAP.”
SOAP Recording Format
S (Subjective) — Subjective Information
・Patient’s complaints and subjective symptoms
・Patient’s own descriptions of changes in condition (e.g., “I feel very sleepy,” “I have no appetite,” “I feel palpitations”)
・Circumstances or lifestyle background leading to the hospital visit
⸻
O (Objective) — Objective Information
・Laboratory test results, vital signs
・Changes or notable points in prescription (new drugs, dose reductions, discontinuation, etc.)
・Observable patient conditions (e.g., complexion, gait, speech)
⸻
A (Assessment) — Evaluation/Consideration
・Pharmacist’s pharmaceutical assessment
・Considerations about drug therapy (interactions, side effect risks, adherence issues)
・Concerns regarding continued use, or points that must be documented
⸻
P (Plan) — Plan
・Contents of the medication guidance provided
・Future instructions or follow-up (e.g., confirm presence of side effects at next visit, check adherence)
・Plans for providing information to the physician when necessary
8) Medication Records Based on “One Problem”
Medication records should be written based on “One problem”. It is essential to clarify the main theme or focus of the guidance given.
This doesn’t mean you must state “this is the main focus” explicitly. Rather, within multiple causal relationships, the key is to identify and document what aspect you intentionally emphasized during guidance. As long as the “One Problem” emerges clearly through the entire SOAP record, it is sufficient.
9) Guidance Amid Complex Backgrounds
The section “A” is where a pharmacist’s true skill is tested. This is where each pharmacist’s knowledge and reasoning distinctly show.
Medication guidance always occurs against complex backgrounds: symptom changes, subjective complaints, and even unrecognized conditions (as is common in chronic disease). A single prescription may involve multiple classes of drugs — antihypertensives, lipid-lowering agents, etc. In such cases, it is crucial to make clear which particular “problem” you chose to focus on during this encounter.
Patients repeatedly return to the pharmacy with new prescriptions. Providing the exact same guidance each time should be avoided. By deliberately approaching from a different angle, previously unseen information may emerge. For example, with a new line of questioning, you may discover unrecorded details about lifestyle or allergies.
Sometimes patients withhold information because they don’t fully trust or understand the pharmacist’s role. That’s why using a different approach, strengthening trust, and even simple daily conversation can enrich communication. This, in turn, makes the medication record more meaningful and alive.
10) Flow of SOAP Documentation
The SOAP format should follow the logical flow: a patient’s chief complaint (S), related objective facts (O), pharmaceutical assessment (A), and the plan (P). This flow ensures a consistent record.
Here is an example produced with ChatGPT:
SOAP Example
S (Subjective):
“Lately I can’t sleep at night. Even with medicine, I have trouble falling asleep.”
O (Objective):
・Current prescription: Zolpidem 5mg at bedtime
・Started 2 weeks ago
・Observed: Slightly tired appearance, no daytime sleepiness
A (Assessment):
・Possibility of insufficient effect. Tolerance or dependence must be considered, but first check adherence and timing of intake.
・Lifestyle factors such as alcohol or caffeine may play a role.
・Any dose adjustment or switching requires physician decision.
P (Plan):
・Confirm intake is at bedtime and emphasize proper timing.
・Advise avoiding caffeine or smartphone use before bed.
・At next visit, confirm efficacy. If no improvement, consider reporting to physician.
This shows how a record becomes a coherent narrative when subjective complaints are paired with objective data, followed by pharmacist’s assessment, and then a plan.
11) Don’t Discard the Long Tail in Medication Records
In reality, not every record will be perfectly coherent. Some patients are unwilling to answer questions. If you insist on rigid structure, you risk omitting valuable information.
Even seemingly “irrelevant” information may later prove useful. For example, a casual remark in the “S” (Subjective) section may become important in future.
Pareto’s Law states that 20% of items account for 80% of outcomes. In medication guidance, perhaps 20% of patient statements directly relate to medicine and account for 80% of importance. However, the remaining “long tail” of information may later become significant.
Dietary habits, lifestyle changes, or job transfers — though not directly related at the time, may later have a major impact. Thus, I recommend documenting even information that appears unrelated.
12) The Core of SOAP
One might wonder: doesn’t including scattered information ruin consistency?
The essential point is that at least “O” (objective facts) and “P” (plans) must be linked.
As in storytelling, the “development” must correspond to the “conclusion.” Records without this alignment fall apart. Like a four-panel comic, the second panel (“development”) and the fourth (“conclusion”) must always correspond.
13) Medication Records Are Tools for Patient Benefit
Another crucial point: medication records are tools, not ends in themselves.
The importance lies not in their structure or narrative, but in how well they serve as tools for communication and guidance.
If a patient is in a hurry and offers little, leave the record as-is for future follow-up. Instead of filling with empty content, document only the facts and use them to connect to future guidance. The critical issue is not the record itself, but the pharmacist’s intent to engage with patient therapy through it.
Even if necessary information cannot be obtained, do not fabricate. Record honestly, leave it as a task for the next visit, and continue from there.
14) Timing of Medication Guidance
When should guidance be given?
A point often overlooked is the organic connection between actual dispensing and the record. If this is ignored, the content of records will drift apart from actual dispensing.
Writing a medication record typically takes at least 5 minutes. It starts during prescription verification — even before meeting the patient. Ideally, when the patient first enters the pharmacy, you ask about circumstances, so pharmaceutical assessment can progress significantly before dispensing.
In reality, however, many pharmacists only meet the patient at the time of dispensing. Thus, drawing inferences from past records and the new prescription becomes crucial. This hypothesis guides the consultation. Without such preparation, guidance becomes improvisational and less effective.
15) Approach with a Hypothesis
This preparation is essentially a “hypothesis.”
Why did the patient visit the hospital? Why this prescription? Here, the pharmacist’s experience shapes their approach. Daily work itself becomes learning.
Sometimes the hypothesis is wrong. Unexpected patient information may emerge. Then the pharmacist must revise the hypothesis and reassess.
Important follow-up points for next time should also be written down for future records.
16) Have a Philosophy as a Pharmacist
Pharmacists write about 30 such records per day. This is demanding. That is why one must have a personal “philosophy” about documenting records.
Here, “philosophy” means an intellectual framework that gives meaning to the act of documentation and a way of thinking that makes medication guidance fruitful practice.
One must step back, reflect, and then put it into practice. To do so, understand SOAP as a framework and adapt it into your own perspective.
If this article helps you in that process, I will be glad.